Unmet medical need
Addressing unmet medical needs of patients through innovation is at the heart of everything we do. Take just some of the recent advances in patient care.
In 2020, 13,437 women across Europe died of cervical cancer. But innovation is fighting back, with the HPV vaccine reducing risk of cervical cancer by 90%. It’s preventing millions of families from losing a sister, daughter, or mother.
Around 15 million Europeans are living with HEP C. But through an innovative course of medicine, we can make that a thing of the past for 95% of patients. Swapping a lifetime of care, for a lifetime of memories.
Incremental advances in the treatment of multiple sclerosis have delivered new medicines and new modes of delivery, making it possible to reduce complications and delay the development of disabilities.
Unmet medical need as a policy making tool
The concept of unmet medical need (UMN) plays an important role in decision making by a range of stakeholders, including regulators, HTA agencies, payers, academics and the pharmaceutical industry. It informs investment and the setting of priorities. Identifying a particular condition or disease area as an UMN is intended to signal its health policy significance, stimulate research activities and incentivise the development of innovative treatments in these areas. Incentives associated with the identification of an UMN can take the form of preferential access to public research funds, access to alternative or accelerated regulatory pathways, consideration of UMN as a value element in HTA, and financial incentives or innovative payment models in reimbursing the health benefits a new treatment delivers.
Introducing a narrow definition of unmet need is challenging
Defining unmet need is personal. Patients living with chronic conditions will define their unmet needs very differently to people facing a life-limiting disease. For long-term conditions, how medicines fit in to daily life is critical, including reduced side-effects, whereas if you are facing a terminal illness you may value extension of life above all else, others may prioritise freedom from pain. Health systems may value treatments that reduce the burden on secondary care more than treatments delivered in hospital. It underlines the need to ensure that a broad range of stakeholders and particularly the patients’ voice is included in any process to define and use unmet need as a policy tool.
Why a narrow definition of UMN hampers research and development
Understanding the nature of innovation, how and where it happens, is critical to addressing unmet needs. The development of medicines takes many years and is always driven by an ambition to address an UMN. However, it is impossible to know in advance whether a particular investment in R&D will eventually address a specific UMN. Given the long and risky development timelines, it is possible that a definition of an UMN can change during this period of development. If what is considered an UMN can change after the investment in R&D has been made, or is defined very narrowly, this leads to a lack of predictability of the incentive, weakening its impact and therefore reducing or removing the stimulus for companies to invest in R&D into relevant treatments to meet patients’ needs. Moreover, R&D aimed at addressing a certain disease area could lead to positive developments, and even breakthrough innovation, elsewhere; limiting incentives to certain defined categories therefore disregards the reality of science. There is no better example than the use of mRNA in COVID-19 vaccines. Originally researched as a potential oncology treatment, mRNA was studied for decades with little or no clinical applications, however, only through that research did we have an asset that could be used to protect citizens against the coronavirus.
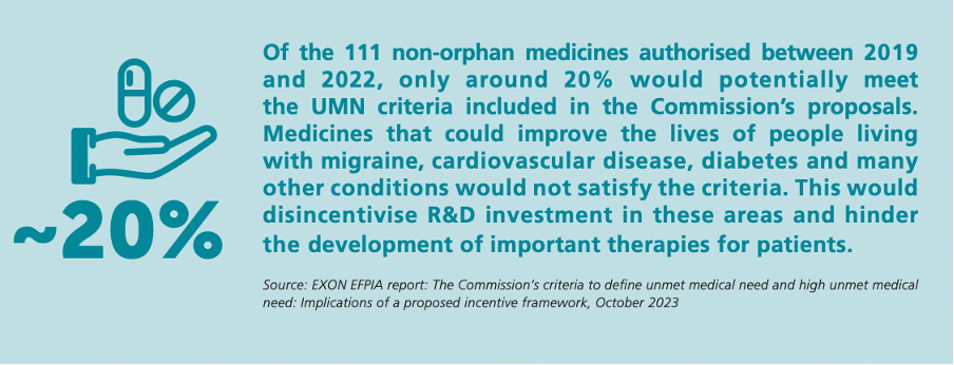
How we define and incentivise medical innovation will shape future waves of medical progress. That is why the conversation about updating the EU’s pharmaceutical legislation is fundamental. Any proposed linkage between RDP protection and development of medicines for UMN risks excluding the development of important therapies for patients. Limiting the definition of UMN to focus only on life-threatening or severely debilitating diseases risks deprioritising conditions that fit neither of these criteria yet have important negative consequences on patients, carers and society. Furthermore, it is unlikely that for any patient population with an unmet medical need, a single medicine will solve that need entirely. More likely, multiple medicines each solve a part of the unmet medical need, either by complementary effectiveness or by differentiation in the part of the patient population that benefits from them. We need a system where the early-stage research and incremental innovation that fuel progress for patients over time are valued and rewarded.
EFPIA’s vision for a European legislative framework that helps direct innovation towards UMN centres on the following guiding principles: